Q-omics provides the consensus-scored PCDH1 profile across patient tissues and cancer cell-line models. PCDH1 expression is associated with patient survival in 25 of 34 cancer types, with the highest sampling consensus in KIRP. Among the 18 cancer types available for tumor–normal comparison, PCDH1 is differentially expressed in 15, with the highest sampling consensus in HNSC. Additionally, PCDH1 protein abundance shows 24,614 significant protein co-abundance associations, with the highest sampling consensus in GBM. Together, these results highlight KIRP, HNSC, and GBM as cancer lineages where PCDH1 shows reproducible signals across survival, tumor–normal expression, and patient cross-omics analyses.
Every result is evaluated using two consensus scores. Sampling consensus measures how consistently a finding is reproduced within a cancer lineage across different conditions. Lineage consensus measures how broadly the result is shared across cancer types, distinguishing pan-cancer signals from lineage-specific patterns.
Premium analyses for PCDH1 — synthetic lethality, tumor antigen, and pembrolizumab response.
This table summarizes PCDH1 survival associations across molecular data types. PCDH1 RNA expression shows survival associations in the most cancer types (25), followed by mutation status (7) and mass-spec protein abundance (6). The rightmost column indicates the cancer type with the highest sampling consensus for each molecular layer.
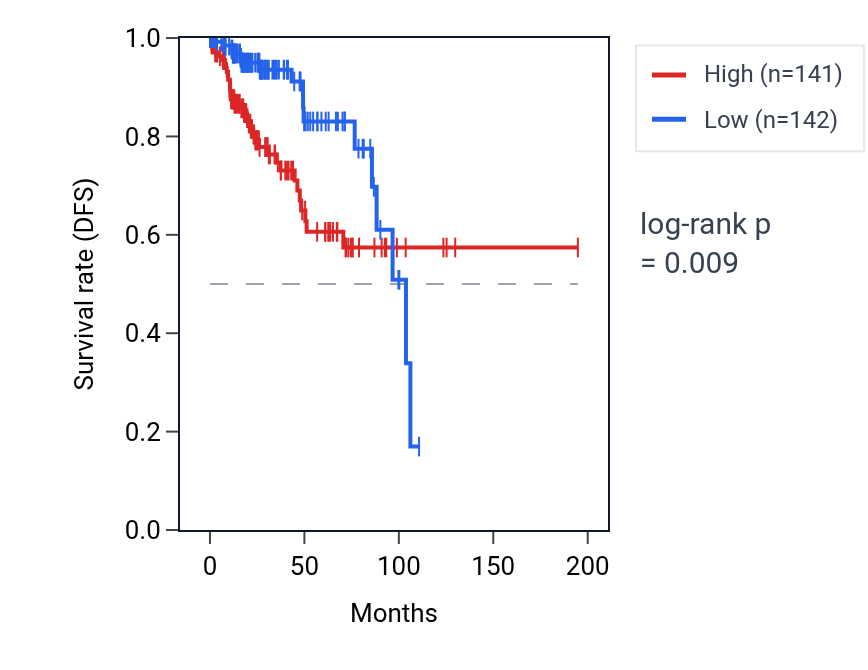
This table ranks reproducible PCDH1 RNA expression–survival associations across cancer types. High PCDH1 expression shows unfavorable associations in KIRP, MESO, PAAD, LUSC and UVM, but favorable associations in KIRC. The KIRP Kaplan–Meier curve shows clear separation, with the high-expression group declining faster, consistent with the unfavorable association (log-rank p < 0.001). Together, the overview and detailed table identify KIRP as the clearest survival context for PCDH1 RNA expression.
This table summarizes PCDH1 tumor–normal expression differences by data type. RNA shows broader differences across cancer types, with a lineage consensus of 15, while mass-spec protein shows differences in 7. The strongest signals are observed in KIRC for RNA and CCRCC for protein.
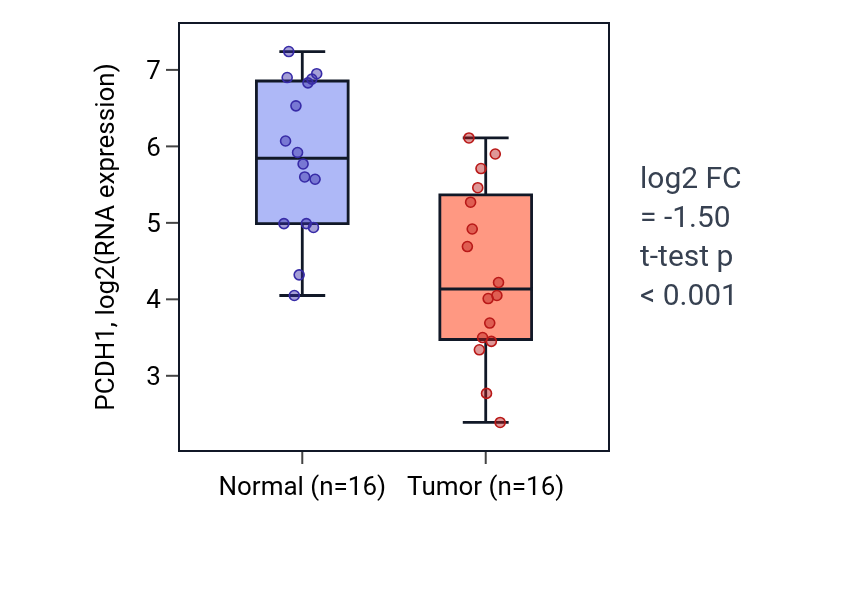
This table ranks reproducible tumor–normal expression differences for PCDH1. A negative fold-change indicates higher expression in normal tissue than in tumor tissue. PCDH1 shows lower tumor expression in HNSC, KIRC, KIRP and LUSC and higher tumor expression in THCA and LIHC. The HNSC box plot shows higher PCDH1 RNA expression in normal versus tumor tissue (log2 FC = −1.504, t-test p < 0.001).
This table shows molecular features associated with PCDH1 in patient tissues and cancer cell lines. In patient samples, PCDH1 shows the broadest associations at the RNA and protein expression levels, with GBM recurring as the lineage with the largest associated feature set. In cancer cell lines, PCDH1 RNA and mutation anchors are most strongly linked to RNA-expression features, especially in BREAST, while CRISPR and shRNA rows add functional-dependency signals in LUNG_NSCLC_LUAD and LARGE_INTESTINE.